
A flexible and practical Normal Physical Exam Template that improves your patients' examinations.
By Ericka Pingol on Jul 15, 2024.
Fact Checked by RJ Gumban.

A physical examination is a crucial component of patient assessment and medical care. It involves a healthcare provider systematically evaluating a patient’s body systems to gather objective data about their health status and the patient's health status. A physical exam aims to identify any signs of disease, injury, or abnormality that may require further investigation or treatment (Garibaldi & Elder, 2021).
The healthcare provider uses various techniques to assess the patient’s overall health and specific body systems during a physical examination. This also helps in informing the patient’s treatment plan.
PDF Template Example PDF
A physical exam is a comprehensive assessment of a patient's health. Here's a breakdown of the critical components:
Performing physical exams is essential for healthcare providers to ensure timely and appropriate patient care. Here are key situations where physical examinations are necessary:
Regular physical exams are fundamental to maintaining health, diagnosing new issues, and managing ongoing conditions. They are a critical component of preventive healthcare and effective medical treatment.
Our Normal Physical Exam template is functional and intuitive. A Normal Physical Exam example is available on this page to help you quickly understand this template. Follow a few steps below to get yourself started with this template:
You can download the free PDF template onto your devices or access it from the Carepatron template library, allowing more flexibility in the template design and content.
Document the necessary patient information for identification purposes. Then, record all the vitals on the template to quickly assess the patient's health status.
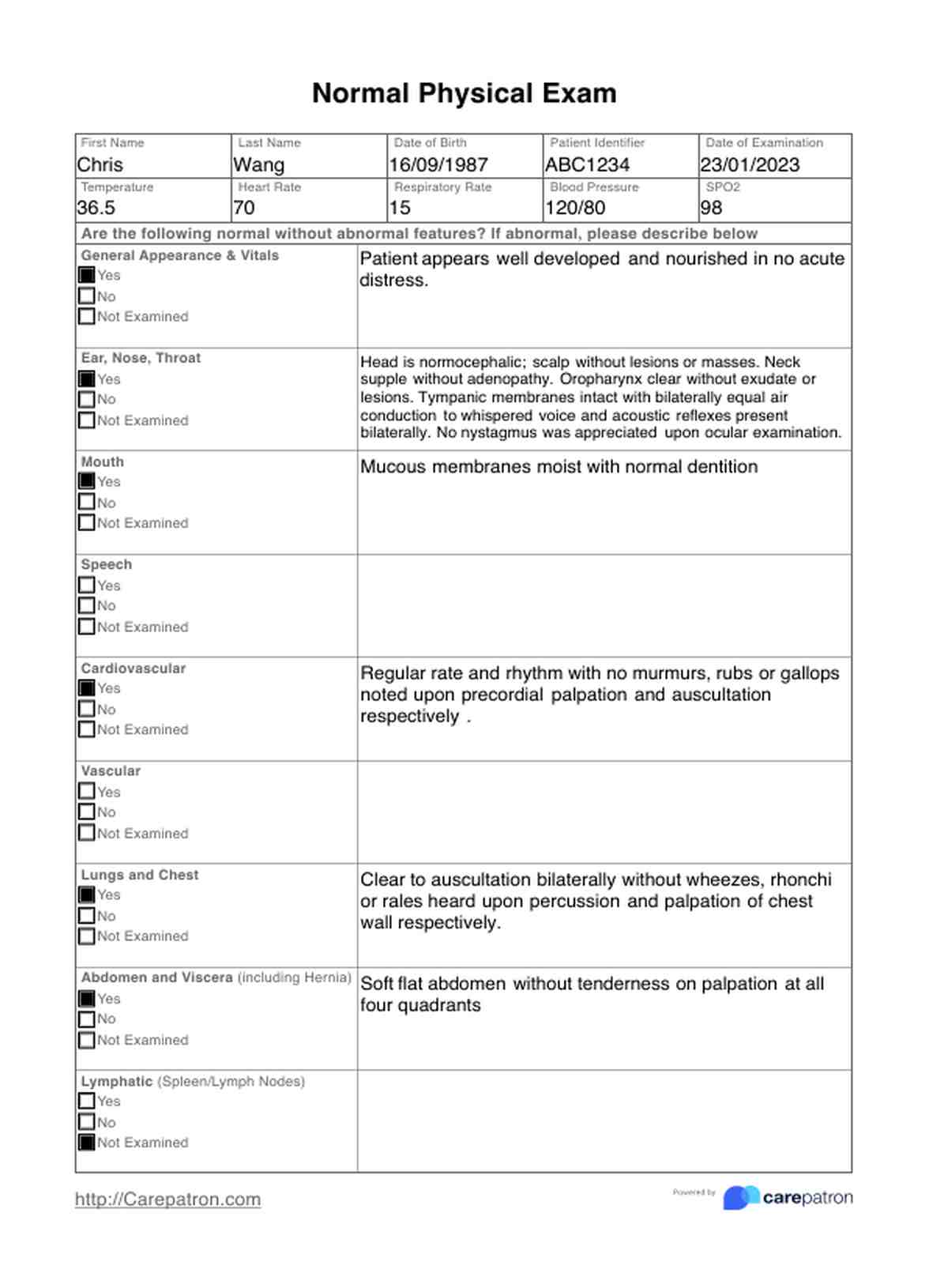
We have listed many systems for you. This certainly doesn't mean you need to assess every body system, only those relevant to the patient's specific presentation. Select and comment on all the reviewed systems, and mark those not examined as ‘not examined.'
You can practically write down anything in this section, from essential documentation of patients’ presenting complaints to highly specialized areas of examination that are not included in the worksheet. Essentially, you are adding anything that brings a holistic picture of the patient to anyone who will view this examination result in the future, aiding in creating the patient's treatment plan.
Once everything is recorded appropriately, you should store this document organized and securely. Due to the confidentiality of the patient and the importance of the information within this document, please treat it with care and professionalism.
When documenting physical exam results, a systematic approach ensures all relevant information is captured accurately and efficiently. Here are key considerations for noting physical exam findings:
Using clear, concise, and objective language is crucial when describing physical exam findings. Avoid ambiguous or subjective terms and use specific, descriptive language to convey the findings accurately. For example, instead of stating "the patient appears tired," document specific observations like "the patient has dark circles under their eyes and yawns frequently during the exam."
Comprehensive physical exam documentation should encompass both normal and abnormal findings. Documenting normal findings establishes a baseline for future reference and demonstrates a thorough examination. When describing abnormal findings, provide specific details such as location, size, shape, color, and texture of any lesions, masses, or abnormalities.
Organizing physical exam findings by body system ensures thorough assessment and documentation of all relevant areas. This systematic approach maintains consistency and completeness in the documentation process. Examples include organizing by HEENT, cardiovascular, respiratory, gastrointestinal, musculoskeletal, and neurological systems.